|
PRACTICAL
SIGNIFICANCE
Few
qualitative
methods
exist to
reliably
identify
abnormal
scapular
motion
(scapular
dyskinesia)
during
an
orthopaedic
clinical
exam.
This
study
introduces
a
reliable
method
of
identifying
scapular
dyskinesia
based on
visual
examination
and also
validates
the
method
by
showing
differences
in
3-dimensional
motion
between
subjects
with and
without
scapular
dyskinesia.
However,
our data
does not
support
a direct
relationship
between
scapular
dyskinesia
and the
presence
of
symptoms
in
athletes
engaged
in
overhead
sports.
STUDY
BACKGROUND
Scapular
dyskinesia
is
believed
to be a
significant
source
of
shoulder
pain and
dysfunction,
particularly
in
athletes
involved
with
overhead
sports;
yet,
clinical
measures
that are
available
to
document
motion
abnormalities
have
questionable
reliability
or are
impractical
for
routine
use.
OBJECTIVE
The
objectives
of this
study
were to
1)
Develop
a
reliable
test for
identifying
scapular
movement
abnormalities
(dyskinesia)
suitable
for
routine
screening
and
clinical
use, 2)
Validate
the test
for
scapular
dyskinesia
using a
previously
validated
motion
analysis
system
to
compare
3-dimensional
motion
between
subjects
judged
as
either
having
or not
having
scapular
dyskinesia.
3)
Determine
the
association
between
abnormal
scapular
movement
and
shoulder
symptoms
in
athletes
engaged
in
overhead
sports.
DESIGN
AND
SETTING
All
measurements
were
performed
in a
laboratory
setting
or at a
protected
area
adjacent
to the
pool.
For
objective
1
(reliability)
all
athletes
were
video-taped
during
testing
to allow
subsequent
evaluation
by
multiple
raters.
For
objective
2
(validity),
66
subjects
initially
rated as
either
clearly
normal
or
obvious
dyskinesia
underwent
instrumented
3-dimensional
motion
analysis.
For
objective
3,
selfreport
data
related
to
symptoms
was
collected
from all
subjects.
SUBJECTS
A total
of 142
athletes
were
tested,
111 male
and 31
females.
The mean
age was
20.8
+/-2.8
years.
Of
these,
49
athletes
represented
baseball,
swimming
or
volleyball
at the
NCAA
Division
III
level.
The
remaining
93
athletes
were
NCAA
Division
I water
polo
players.
Subjects
had to
be
actively
competing
in an
overhead
sport,
and
could
not be
obese
(BMI >
30), or
have a
recent
history
of
rotator
cuff
tear,
dislocation
or
direct
contact
shoulder
injury.
MEASUREMENTS
Raters
were
trained
to
detect
scapular
dyskinesia
using
written
operational
definitions
and
video
examples
of
normal
and
abnormal
motion.
Scapular
dyskinesia
was
defined
as the
presence
of
either
“winging”
(medial
or
inferior
border
of the
scapula
protrudes
≥ 1”
with a
sulcus/gap
present
between
thorax
and
scapula)
or
“dysrhythmia”
(premature
or
excessive
elevation
or
protraction;
or
non-smooth
or
stuttering
motion
during
arm
elevation
or
lowering).
Right
and left
sides
were
rated
independently
for each
test
motion
as
either
“normal”,
“subtle”,
or
“obvious”
dyskinesia.
Two
raters
independently
observed
and
rated
scapular
motion
in all
athletes
performing
the
prescribed
tasks at
the time
of
testing.
Subsequently,
six
raters
(three
pairs)
each
rated 30
subjects
chosen
randomly
(total
90) by
viewing
videos.
A
quantitative
3-dimensional
analysis
was
accomplished
using
electromagnetic
based
sensors
applied
to the
humerus
and
scapula
bilaterally
and to
the
thorax
based on
previously
described
protocols.
Symptoms
were
assessed
using
the
University
of
Pennsylvania
Shoulder
Score
which is
a
composite
based on
pain at
rest,
moderate
activity,
and
strenuous
activity.
Reliability
was
assessed
using
percent
agreement
and
weighted
kappa,
and the
relationship
between
symptoms
and
scapular
dyskinesia
was
evaluated
by odds
ratios.
RESULTS
Percent
agreement
ranged
from
75-86%
and
Kappa
values
(95% CI)
ranged
from
0.46(0.27-0.65)
to 0.67
(0.52-
0.79)
for
dyskinesia
ratings
of each
shoulder
and test
movement.
Significant
differences
in
3-dimensional
scapular
motion
were
found
between
subjects
visually
rated as
normal
compared
to those
rated as
having
dyskinesia.
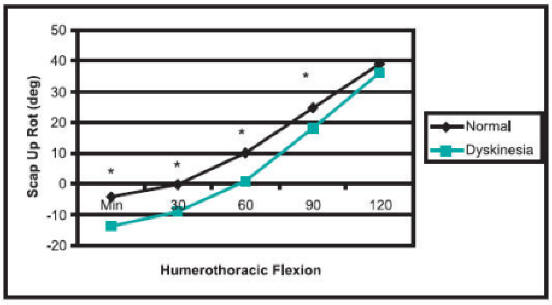
Subjects
with
dyskinesia
had
significantly
less
upward
rotation
(Figure
1), less
clavicle
elevation
and
greater
clavicle
protraction
during
flexion.
The
presence
of
shoulder
symptoms
was not
significantly
different
between
the
“normal”
and
“obvious”
subjects
(Odds
Ratio=0.79,
95%CI:
0.33
-1.89).
CONCLUSIONS
The test
for
scapular
dyskinesia
shows
satisfactory
reliability
for
clinical
use.
Subjects
visually
judged
as
having
dyskinesia
generally
have
less
upward
rotation
and
clavicle
elevation
and
greater
clavicle
protraction
during
flexion.
The
presence
of
scapular
dyskinesia
was not
related
to
shoulder
symptoms
in
athletes
engaged
in
overhead
sports.
|
|
| Figure 1. Subjects visually rated as having dyskinesia demonstrated significantly less scapular upward rotation compared to those judged as normal. |
Funded
by NFL
Charities
|
Publication
&
Presentation
List:
-
McClure
PW,
Kareha
SM,
Tate
AR,
Irwin
D,
Stuckey
E.
Reliability
of a
clinical
test
to
detect
scapular
dyskinesia
and
its
relationship
to
shoulder
symptoms
in
athletes.
NATA
Annual
Meeting
and
Clinical
Symposium,
Atlanta,
GA,
June
2006
|
|
|
|

Philip W. McClure, PhD, PT
Principal Investigator |
Dr. McClure is an Professor, Department of Physical Therapy at Arcadia University. He also practices at Penn Therapy and Fitness, an outpatient clinic affiliated with the University of Pennsylvania Medical Center. He received his B.S. in Physical Therapy from Temple University in 1982, his M.S. in Orthopedic Physical Therapy from Medical College of Virginia in 1987, and his PhD in Biomedical Science from Drexel University in 1996.
Philip W. McClure, PhD, PT
Arcadia University
450 S. Easton Road
Glenside, PA 19038
215-572-2863
mcclurep@arcadia.edu |
|
|
This
Grant
Information
Summary
may be
downloaded
in a
2-page
pdf file
from
www.natafoundation.org/pdfs/McClurePhillip.pdf. |
Back to
March 9, 2010
eBlast
Newsletter
Send e-mail
to teresa@nata.org with questions
or
comments
about this web site. |