|
PRACTICAL
SIGNIFICANCE
Gaining
full
comprehension
of the
joint
mechanics
in knee
OA
patients
during
stair
climbing
is
essential
for
understanding
functional
deficits,
providing
optimal
treatment
and
rehabilitation,
as well
as
extending
the
quality
of life
in
patients
that
suffer
from
this
debilitating
disease.
STUDY
BACKGROUND
Osteoarthritis
(OA) is
a common
musculoskeletal
condition
affecting
an
estimated
27
million
Americans.
Specifically,
tibiofemoral
joint OA
is the
most
common
form due
to the
consistent
joint
loading
the knee
joint
complex
receives
throughout
one’s
lifespan.
We are
entering
an era
where
knee OA
is being
diagnosed
in
epidemic
proportions;
further,
it is
becoming
more
evident
that
further
research
is
needed
to fully
understand
lower
extremity
joint
mechanics
during a
common
daily
task
such as
stair
climbing
in
patients
who
suffer
from
knee OA.
Not only
is
gaining
a better
understanding
of how
knee OA
directly
influences
knee
joint
mechanics
during
stair
gait
critical,
but so
too is
understanding
how hip
and
ankle
joint
mechanics
may also
be
affected
during
stair
gait.
OBJECTIVE
To
compare
various
hip,
knee and
ankle
joint
kinematic
variables
between
knee OA
subjects
and
matched
healthy
controls
during
stair
ascent
and
descent.
DESIGN
AND
SETTING
A
case-controlled,
crossover
design
was used
to study
subjects
performing
5
ascending
and
descending
stair
gait
trials
while
lower
extremity
joint
motion
was
captured
three
dimensionally
in a
Biodynamics
Research
Laboratory.
SUBJECTS
Eighteen
subjects
with
knee OA
(age
60.17 ±
9.98
yrs,
mass
90.27 ±
16.73
kg, ht
168.41 ±
9.92 cm)
and 18
healthy
matched
controls
(age
60.28 ±
10.66
yrs,
mass
81.12 ±
21.21
kg, ht
168.28 ±
11.95
cm)
participated
in the
study.
MEASUREMENTS
Sagittal
and
frontal
plane
hip,
knee and
ankle
kinematics:
average
angle at
foot
strike
(°),
peak
angle
during
support
(°),
time of
peak
angle
during
support
(%),
peak
angle
during
swing
(°),
time of
peak
angle
during
swing
(%) and
average
angle at
toe off
(°)
during
stair
ascent
and
stair
descent
was
measured
using an
optical
video
motion
capture
system
(Figure
1).
RESULTS
Significant
group by
direction
interactions
were
found
for
average
hip
flexion
angle at
foot
strike [P
=
0.041],
average
ankle
adduction
angle at
foot
strike [P
=0.007],
and peak
ankle
dorsiflexion
angle
during
swing [P=
0.015].
Specifically,
knee OA
and
control
subjects
demonstrated
greater
hip
flexion
angle at
foot
strike
and
ankle
dorsiflexion
angle
during
swing
during
stair
ascent
compared
to
descent.
Further,
knee OA
patients
demonstrated
greater
hip
abduction
at foot
strike
(-3.08°
± 3.94)
and
smaller
peak
knee
flexion
during
swing
(86.73°
± 5.43).
The time
of peak
hip
abduction
(34.18%
± 7.07),
peak
knee
flexion
(69.84%
± 4.57)
and peak
ankle
adduction
(37.27%
± 20.77)
during
support
and the
time of
peak hip
flexion
(85.22%
± 3.7),
peak
knee
flexion
(77.67%
± 3.75)
and
ankle
dorsiflexion
(80.73%
± 4.50)
angle
during
swing
occurred
later in
the gait
cycle
for knee
OA
patients
compared
to
control
subjects.
Figures
2 & 3
demonstrate
knee
joint
kinematics
during
stair
ascent
and
descent.
CONCLUSIONS
These
data
demonstrate
that
knee OA
directly
influences
specific
knee
joint
kinematics.
Pathological
deviations
at the
knee
appear
to
induce
kinematic
alterations
at the
hip and
ankle
perhaps
in an
effort
to
compensate
for the
existing
knee
joint
pathology.
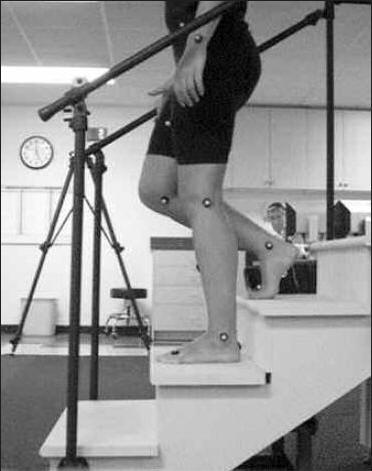
Figure
1:
Customized
staircase
used for
lower
extremity
3D joint
kinematic
analysis
during
stair
ascent
and
descent.
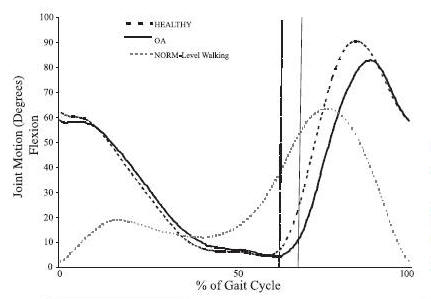
Figure
2:
Average
Sagittal
Plane
Knee
Joint
Displacement
During
Stair
Ascent
NB:
Hashed
and
solid
vertical
lines
indicate
end of
support
time for
healthy
and OA
subjects,
respectively
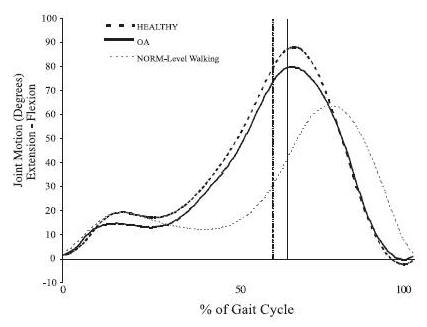
Figure
3:
Average
Sagittal
Plane
Knee
Joint
Displacement
During
Stair
Descent
NB:
Hashed
and
solid
vertical
lines
indicate
end of
support
time for
healthy
and OA
subjects,
respectively
|
Publication
&
Presentation
List:
-
Hicks-Little CA, Peindl RD, Hubbard TJ, Scannell BP, Springer BD, Odum SM, Fehring,TK, Cordova ML. Knee Osteoarthritis Induces Alterations in Lower Extremity Joint Kinematics during Stair Ascent and Descent. NATA Annual Meeting & Clinical Symposia, San Antonio, Texas June 2009
|
|
|
|

Charlie A. Hicks-Little, PhD, ATC
Principal Investigator
|
Charlie A. Hicks-Little, PhD, ATC
Dr. Charlie Hicks-Little received her BS in Athletic Training and MS in Exercise Science with an emphasis in Sports Medicine from East Stroudsburg University of Pennsylvania. She received her Ph.D in Biomedical Science from the University of North Carolina at Charlotte. Charlie is an Assistant Professor in the Department of Exercise and Sport Science at the University of Utah, where she teaches undergraduate courses in the Athletic Training Education Program and graduate courses in the Sports Medicine Program. She is the Director of the new Sports Medicine Research Laboratory, and also directs the Sports Medicine Graduate Program. Charlie’s areas of research interest include investigating the mechanical, sensorimotor and neuromuscular effects of knee osteoarthritis. It is through this research that she aspires to positively influence therapeutic paradigms in the rehabilitation of degenerative knee joint disease that affects many worldwide.
|
|
|
This
Grant
Information
Summary
may be
downloaded
in a
2-page
pdf file
from
http://www.natafoundation.org/wp-content/uploads/2012/11/Hicks-Little09.pdf |
Back to
November 14, 2012
eBlast
Newsletter
Send e-mail
to rachaelo@nata.org with questions
or
comments
about this web site. |